थ्रोम्बोलिसिस
थ्रोम्बोलिसिस
By Dr.Ravindra Patil
रक्त हा आपल्या शरीराचा एक जादुई अवयव आहे जो आपल्या शरीरात धमन्यांमधून आणि शिरांमधून आयुष्यभर वाहत राहतो. रक्त फुफ्फुसातून आवश्यक असलेल्या सर्व ऊतींमध्ये ऑक्सिजन वाहून नेते आणि सर्व उतींमधून कार्बन डायऑक्साईड परत फुफ्फुसात वाहून नेते. हे शरीराच्या प्रत्येक पेशीचे पोषण करते आणि सर्व उती आणि अवयवांमधून टाकाऊ पदार्थ बाहेर टाकण्यासाठी मूत्रपिंडात वाहून नेले जाते. हे आपण हायस्कूलच्या विज्ञान वर्गात शिकतो.
शाळेत असताना आपण सगळेच स्वतःला इजा करून घेतो. आपली त्वचा फाटू शकते आणि आपल्याला रक्तस्त्राव होऊ शकतो. पण आपल्या जादुई रक्ताच्या विशेष गुणांमुळे रक्त गोठते व पुढील रक्तस्त्राव थांबतो. हे आपण सर्वांनी अनुभवले आहे.
निरोगी लोकांच्या रक्ताची जादू अशी आहे की, दुखापत झाल्यावरच ते गोठते व आपला रक्तस्त्राव थांबतो. रक्त गोठण्यामुळे शरीरातून अधीक रक्त वाया जात नाही. निरोगी लोकांमध्ये, रक्त कधीही धमन्या, नसा किंवा हृदयात गोठत नाही किंवा त्याच्या गाठी होत नाहीत. ते नेहमी द्रव अवस्थेत राहते. आणि नमूद केल्याप्रमाणे आपला रक्त पुरवठा प्राणवायु आणि पोषक तत्वे पुरवण्याचे आणि टाकाऊ पदार्थ आणि कार्बन डायऑक्साइड बाहेर काढण्याचे सतत काम करत असतो. जर रक्ताच्या गुठळ्यामुळे अचानक रक्त वाहणे थांबले, तर प्रभावित अवयवांना प्रथम ऑक्सिजनची उपासमार होईल आणि थोड्याच वेळात त्या अवयवांचा मृत्यू होऊ शकतो.
मेंदू किंवा हृदय या अवयवांवर परिणाम झाला तर तो माणूसच मरेल!
त्यामुळे रक्त कोणत्याही किंमतीत द्रव अवस्थेत राहिले पाहिजे व वाहत राहिले पाहिजे.
Table of Contents
थ्रोम्बोसिस आणि एम्बोलिझम
तथापि, काही प्रसंगी वेगवेगळ्या रोगापूर्वीच्या घटकांमुळे, रक्तवाहिन्यामध्ये रक्ताच्या गुठळ्या होतात. याला थ्रोम्बोसिस असे म्हणतात.
या गुठळ्या काहीवेळा तुटतात, बाहेर पडतात आणि रक्ताभिसरण प्रणालीच्या दूरच्या भागात जातात, तिथे त्या अडकतात आणि त्या पुढील रक्तपुरवठा रोखतात. याला एम्बोलिझम म्हणतात.
कधीकधी थ्रोम्बोसिस आणि एम्बोलिझम दोन्ही एकत्र होतात आणि नंतर त्याला थ्रोम्बो-एम्बोलिक घटना म्हणून ओळखले जाते.
जर रक्तवाहिनी शीरे मध्ये गुठळी तयार झाली आणि ती सैल झाली व तिचा तुकड पडला, तर तो फुफ्फुसांच्या धमन्यांपर्यंत नेला जाईल आणि त्यांना फुफ्फुसांच्या धमनीला ब्लॉक करेल. याला पल्मोनरी एम्बोलिझम म्हणतात आणि ही एक अतिशय गंभीर व जीवघेणी स्थिती आहे.
वरील सर्व प्रकरणांमध्ये, मानवी शरीराच्या धमन्यांमध्ये रक्ताची गुठळी झाली आहे, ज्यामुळे त्या धमनीद्वारे पुरवल्या जाणार्या अवयवांची उपासमार होते व तो अवयव मरू शकतो. पण वरी रक्ताच्या गुठळ्या असलेल्या धमन्या जर हृदयाला किंवा मेदूला रक्तपुरवठा करत असल्या तर ती व्यक्ती गंभीर आजारी पडू शकते किंवा मृत्यू देखील पाऊ शकते.
इतर सर्व अवयवांचा रक्तपुरवठा ठप्प झाला तर परिणाम वाईटच होतो, परंतु हृदय किंवा मेंदूच्या रक्तपुरवठ्यात अडथळा आल्यास त्वरित मृत्यू होऊ शकतो.
पक्षघाताच्या (लकवा किंवा इंग्रजीत ज्याला स्ट्रोक म्हणतात त्या रूग्णांना) रूग्णांना थ्रोम्बोलिसिस हा उपचार सर्वोत्तम उपचारांपैकी एक आहे.
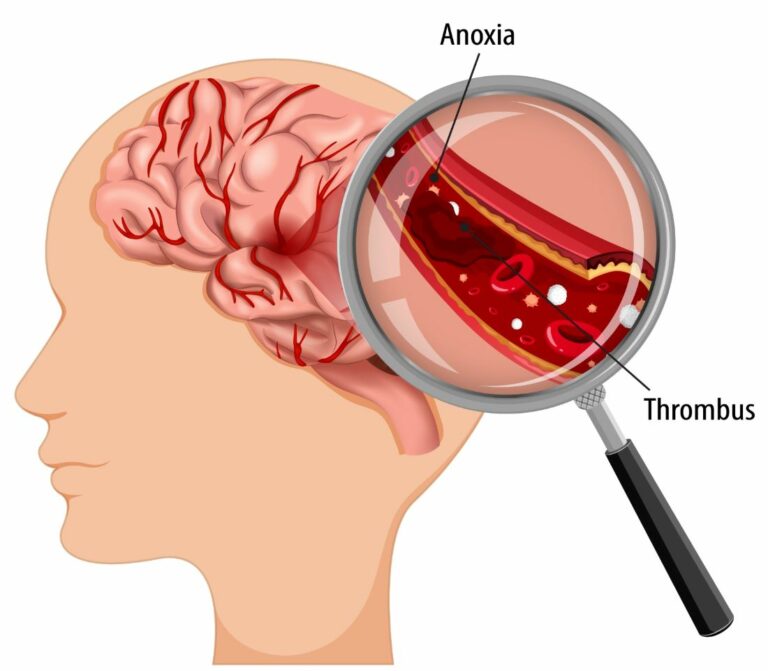
मेंदूच्या धमनीत गुठळ्या झाल्यामुळे सेरेब्रोव्हस्कुलर स्ट्रोक किंवा ब्रेन स्ट्रोक नावाचा तीव्र आजार होतो.
हृदयाच्या धमनीत गुठळ्या झाल्यामुळे मायोकार्डियल इन्फार्क्शन किंवा हृदयविकाराचा झटका म्हणून ओळखला जाणारा एक तीव्र रोग होतो.
फुफ्फुसाच्या धमन्यांमधील गुठळ्याला पल्मोनरी एम्बोलिझम असे म्हणतात.
थ्रोम्बोलिसिस
सोप्या शब्दात, थ्रोम्बोलिसिस [थ्रॉम्बोलाइटिक थेरपी म्हणूनही ओळखले जाते] रक्तवाहिन्यांमधील धोकादायक गुठळ्या विरघळवणे, रक्त प्रवाह सुधारणे आणि ऊती आणि अवयवांना होणारे नुकसान टाळण्यासाठी हा उपचार आहे. थ्रोम्बोलिसिस म्हणजे गुठळ्या विरघळवणाऱ्या औषधे इंट्राव्हेनस इंजेक्शनद्वारे किंवा लांब कॅथेटरद्वारे शीरेत इंजेक्शने दिली जातात व जी थेट ब्लॉकेजच्या ठिकाणी औषधे पोहोचवतात.
हे एका लांब कॅथेटरच्या टोकाला जोडलेल्या यांत्रिक उपकरणाने कॅथ लॅब मध्ये देखील केले जाऊ शकते. या प्रकारात एकतर गठ्ठा काढून टाकतात किंवा तो हळुहळु तोडतात.
थ्रोम्बोलिसिस प्रक्रियेचा उपयोग हृदय व मेंदूला रक्तप्रवाह देणाऱ्या धमन्यांमध्ये रक्ताच्या गुठळ्या विरघळवण्यासाठी आणीबाणीच्या उपचार म्हणून केला जातो – हृदयाच्या धमन्यांमध्ये क्लॉट झाला तर हृदयविकाराचा झटका येतो आणि मेंदूच्या धमनीत क्लॉट झाला इस्केमिक स्ट्रोकचे होतो. त्या शिवाय फुफ्फुसांच्या धमन्यांमध्ये क्लॉट झाला तर त्याला पल्मोनरी एम्बोलिझम म्हणतात व तेथे पण थ्रोम्बोलिसिस प्रक्रिया वापरून उपचार करतात.
खालील भागात देखील रक्ताच्या गुठळ्यांवर उपचार करण्यासाठी थ्रोम्बोलिसिस प्रक्रिया वापरली जाते:
- शिरांच्या (व्हेन्सच्या आत) आत: याला डीप व्हेन थ्रोम्बोसिस (डी.व्ही.टी.) असे म्हणतात. हे पायांच्या नसा, ओटीपोटाचा भाग आणि वरच्या बाजूला असलेल्या नसांमधील गुठळ्या असतात; उपचार न केल्यास, गुठळ्याचे तुकडे फुटू शकतात आणि फुफ्फुसातील धमनीमध्ये जाऊ शकतात, परिणामी तीव्र पल्मोनरी एम्बोलिझम होतो.
- बायपास ग्राफ्ट्सच्या आत: या म्हणजे हृदयाच्या बायपास शस्त्रक्रियेमध्ये वापरल्या जाणार्या नसांमध्ये तयार झालेल्या गुठळ्या आहेत, हृदयविकाराच्या उपचारासाठी केल्या जातात. या शिरा रुग्णाच्या पायातून काढल्या जातात. या नसांमध्ये रक्ताची गुठळी झाल्यास हृदयविकाराचा दुसरा झटका येऊ शकतो.
- डायलिसिस कॅथेटर्सच्या आत: ज्या रुग्णांना वारंवार डायलिसिसची गरज असते त्यांच्या मानेच्या शिरामध्ये या जीवनरक्षक नळ्या घातल्या जातात. अशा नळीच्या आत गुठळी असणे म्हणजे रुग्णाला डायलिसिस करता येत नाही आणि अत्यंत गंभीर स्थिती उद्भवते.
जर रक्ताची गुठळी जीवघेणी ठरली असेल आणि हृदयविकाराचा झटका, स्ट्रोक किंवा पल्मोनरी एम्बोलिझमचे निदान झाले असले तर – शक्य तितक्या लवकर उपचार करता आला– आदर्श रीते एक ते दोन तासांच्या आत – तर थ्रोम्बोलिसिस हा उपचाराचा उत्तम पर्याय असतो. सुरू केल्यास एक पर्याय असू शकतो
थ्रोम्बोलिसिसची विविध औषधे
सर्वात सामान्यपणे वापरल्या जाणारी क्लोट-बस्टिंग औषधे — ज्यांना थ्रोम्बोलाइटिक एजंट्स किंवा थ्रोम्बोलिसिस इंजेक्शन्स देखील म्हणतात – ती खालील प्रमाणे आहेत:
- एमिनेस (एनिस्ट्रेप्लेस)
- रेटावेस (रेटीप्लेस)
- स्ट्रेप्टेज (स्ट्रेप्टोकायनेज, काबिकिकायनेज)
- टी-पीए (औषधांचा वर्ग — ज्यामध्ये अॅक्टिव्हेस समाविष्ट असते)
- टी एन केस (टेनेक्टेप्लेस)
- अॅबोकिनेज, किनलायटिक (रोकिनेज)
परिस्थितीनुसार डॉक्टर कॅथेटरद्वारे ऍक्सेस साइटमध्ये क्लॉट-बस्टिंग औषधे इंजेक्ट करू शकतात. तथापि, बहुतेकदा, डॉक्टर रक्तवाहिनीमध्ये एक लांब कॅथेटर घालतात आणि रक्ताच्या गुठळ्यांजवळ औषधे थेट गुठळ्यांपर्यंत पोहोचवतात.
दोन्ही प्रकारच्या थ्रोम्बोलिसिस दरम्यान, रक्ताची गुठळी विरघळत आहे की नाही हे पाहण्यासाठी डॉक्टर रेडिओलॉजिक इमेजिंग वापरतात. जर गठ्ठा तुलनेने लहान असेल तर प्रक्रियेस अनेक तास लागू शकतात. परंतु गंभीर अडथळ्यासाठी अनेक दिवस उपचार आवश्यक असू शकतात.
थ्रोम्बोलिसिस केव्हा करू नये
जरी थ्रोम्बोलिसिस सुरक्षितपणे करता येते आणि त्यामुळे प्रभावीपणे रक्त प्रवाह सुधारू शकतो आणि अधिक आक्रमक शस्त्रक्रियेशिवाय अनेक रुग्णांमध्ये लक्षणे दूर करू शकतो तरी खालील प्रकरणांमध्ये थ्रोम्बोलिसिस केले जाऊ शकत नाही:
- उच्च रक्तदाब
- सक्रिय रक्तस्त्राव किंवा रक्त कमी होणे
- मेंदूमध्ये रक्तस्त्राव झाल्यामुळे पक्षघात
- मूत्रपिंडाचा गंभीर आजार
- अलीकडे झालेली शस्त्रक्रिया
- गरोदरपण
- वृध्ध रुग्णांमध्ये
गंभीर अंतर्गत रक्तस्त्राव होण्याच्या जोखमीव्यतिरिक्त, थ्रोम्बोलिसिसच्या इतर संभाव्य जोखमींमध्ये खालील धोके समाविष्ट आहेत:
- जेथून थ्रोम्बोलिसि साठी सुई घालतात त्या ठिकाणी जखम होणे किंवा रक्तस्त्राव होणे
- रक्तवाहिनीला नुकसान
- रक्ताच्या गुठळ्याचे रक्तवहिन्या मार्गे दुसर्या भागात स्थलांतर
- मूत्रपिंडाचे नुकसान व आजार
सर्वात गंभीर संभाव्य गुंतागुंत म्हणजे इंट्राक्रॅनियल रक्तस्त्राव, परंतु हे होणे दुर्मिळ असते.
थ्रोम्बोलिसिस केल्या नंतर रूग्णाचे भविष्य
थ्रोम्बोलिसिस सहसा जरी यशस्वी होत असले तरी, 25% रुग्णांमध्ये रक्ताची गुठळी विरघळण्यास उपचार सक्षम होत नाही. आणखी 12% रुग्णांच्या रक्तवाहिनीत गुठळ्या किंवा अडथळे पुन्हा विकसित होतात.
याव्यतिरिक्त, केवळ थ्रोम्बोलायसिस – यशस्वी असतानाही – आधीच रक्त प्रवाह बंद झाल्यामुळे आधीच खराब झालेल्या ऊतींवर उपचार करता येत नाहीत. त्यासाठी अधीक उपचारांची आवश्यकता असू शकते.
स्ट्रोकच्या रूग्णांना थ्रोम्बोलिसिस उपचार
मिरजेच्या समर्थ न्यूरो आणि सुपरस्पेशालिटी हॉस्पिटल सारख्या प्रगत मेंदू उपचार रुग्णालयांमध्ये, स्ट्रोकच्या रूग्णांमध्ये थ्रोम्बोलायसीस अतिशय विशिष्ट पद्धतीने केले जाते. स्ट्रोकचा रूग्ण हॉस्पिटलमध्ये येत असल्याची माहिती रुग्णालयाला मिळताच आपत्कालीन कक्ष आणि सीटी स्कॅन कक्ष सज्ज ठेवण्यात येतात. रुग्णाला सीटी स्कॅन रूममध्ये पोहोचवल्यानंतर मेंदूची सीटी स्कॅन तपासणी केली जाते. मेंदूमध्ये रक्ताची गुठळी आढळल्यास रिकॉम्बिनंट टिश्यू प्लास्मिनोजेन अॅक्टिव्हेटर [rtPA] या औषधाने त्वरित उपचार सुरू केले जातात आणि सतत बारीक निरीक्षण करण्यासाठी रुग्णाला आय.सी.यु. मध्ये स्थानांतरित केले जाते.
जर रुग्ण “गोल्डन अवर” मध्ये आला असेल किंवा स्ट्रोकनंतर पहिल्या ६० मिनिटांत आला असेल तर, रुग्ण स्ट्रोकमधून अगदी कमी वेळात पूर्णपणे बरा होण्याची शक्यता असते.


