त्याला मणक्यात दोनदा ट्यूमर झाले पण सर्जिकल नेव्हिगेशनने वाचवले

त्याला मणक्यात दोनदा ट्यूमर झाले पण सर्जिकल नेव्हिगेशनने वाचवले
By Dr.Ravindra Patil
समर्थ न्यूरो आणि मल्टीस्पेशालिटी हॉस्पिटल [मिरज, पश्चिम महाराष्ट्र] चे मुख्य न्यूरोसर्जन डॉ रवींद्र पाटील, त्यांनी सर्जिकल नेव्हिगेशनच्या मदतीने केलेल्या एक कठीण केस विषयी माहिती सांगत आहेत…
महंतेश शेलीकेरी हे मूळचे बेळगावचे आहेत. त्यांना न्यूरोफायब्रोमेटोसिस नावाचा दुर्मिळ आजार होता. त्याच्या पाठीत पाठीच्या कण्यावर दोन गाठी झाल्या होत्या व त्या स्पायनल कॉर्डवर दाब देत होत्या. त्यामुळे दोन महिन्यांपासून त्याची चालण्याची क्षमता कमी झाली होती.
Table of Contents
न्यूरोफिब्रोमेटोसिस
Neurofibromatosis (NF) ही अशी परिस्थिती आहे ज्यामध्ये मज्जासंस्थेमध्ये ट्यूमर वाढतात. न्यूरोफिब्रोमॅटोसिसचे तीन प्रकार आहेत, प्रकार I (NF1), प्रकार II (NF2) आणि श्वानोमॅटोसिस. NF मधील ट्यूमर सामान्यतः कर्करोग नसलेल्या असतात.
कर्करोगाच्या गाठींच्या तुलनेत कर्करोग नसलेल्या ट्यूमर अर्थातच चांगले असतात, कारण ते वेगाने वाढत नाहीत आणि शरीराच्या इतर भागात पसरत नाहीत. पण महांतेशचे दुर्दैव असे की त्याला पाठीच्या कण्यामध्ये NF ट्यूमर होता. 13 वर्षांपूर्वी NF ट्यूमर काढण्यासाठी त्याच्या कमरेच्या मणक्यामध्ये शस्त्रक्रिया करण्यात आली होती. शल्यचिकित्सकाने दुस-या लंबर कशेरुका [L2] च्या स्तरावरील ट्यूमर काढला होता. पण महांतेशसाठी दुःखाची गोष्ट म्हणजे, न्यूरोफिब्रोमेटोसिस ट्यूमर पुनरावृत्ती झाली! यावेळी ते 12 व्या थोरॅसिक कशेरुका [T12] आणि प्रथम लंबर मणक्यांच्या [L1] वर होते.
ट्यूमर पुन्हा वाढल्यामुळे, महांतेशला खालच्या अंगात दोन्ही बाजुला अशक्तपणा आला. गाठी वाढत गेल्याने हळूहळू त्याला चालता येत नव्हते. त्याच्या एम.आर.आय. स्कॅनमध्ये T12, L1 आणि L2 मणक्यांच्या स्तरावर एकापेक्षा जास्त स्पाइनल ट्यूमर दिसून आले. त्यामुळे त्याला न्यूरोसर्जनकडे पाठवण्यात आले. न्यूरोसर्जनने स्पष्ट केले की शस्त्रक्रिया अत्यंत जोखमीची होती कारण ट्यूमर लहान होते आणि ते अचूकपणे शोधणे कठीण होते आणि ते काढताना महांतेशला त्याच्या खालच्या अवयवांना कायमचा अशक्तपणा किंवा अर्धांगवायू आणि मूत्राशय आणि आतड्यांवरील नियंत्रण आंशिक किंवा पूर्ण नुकसान होण्याची शक्यता होती.
आणि जर महांतेशवर लवकर शस्त्रक्रिया केली नसती, तरीही त्याला कायमचा अशक्तपणा किंवा खालच्या अंगाचा अर्धांगवायू आणि मूत्राशय आणि आतड्यांवरील नियंत्रण अर्धवट किंवा पूर्ण गमावण्याची शक्यता होती!
इकडे आड आणि तिकडे विहीर अशी परिस्थिती महांतेशवर आली होती.
त्यांच्या जीवनात आणखी एक गुंतागुंत होती. महांतेशच्या पत्नीला पोलिओमायलाइटिस आहे. ती दिव्यांग गटात आहे. चालताना तिला काठी लागते. त्यामुळे जर महांतेशला पॅराप्लेजिया झाला असता तर ती त्याला जगण्यास मदत करण्यास सक्षम नव्हती.
याशिवाय, शस्त्रक्रियेचा खर्च हा मोठा प्रश्न होता.
त्यामुळे महांतेश शेल्लिकेरी आणि त्यांची पत्नी खरोखरच हताश परिस्थितीत होते. त्यांच्या असहाय्य परिस्थितीत त्यांच्या कुटुंबाने त्यांना खूप मदत केली.
महांतेशच्या उपचारासाठी अनेक न्यूरोसर्जनचा सल्ला घेण्यात आला. सर्वांनी त्यांना समजावून सांगितले की शस्त्रक्रिया ही एक धोकादायक पायरी आहे कारण महांतेशला पूर्ण पॅराप्लेजिया आणि मूत्राशय तसेच आतड्यांसंबंधी असंयम होण्याची दाट शक्यता होती.
योगायोग आणि संयोग
महांतेशच्या नातेवाईकांपैकी एक जण डॉक्टर आहेत. ते डॉ. सोमनाथ खेराडकर यांना भेटले, त्यांनी दुसरे मत (सेकंड ओपिनियन) घेण्यासाठी माझे नाव सुचवले.
जेव्हा महांतेश आणि कुटुंब माझ्याकडे आले तेव्हा ते खूप घाबरलेले आणि हताश होते. त्याची तब्बेत सुधारेल अशी त्याची फारशी आशा नव्हती. म्हणून सर्वप्रथम मी त्यांना धीर दिला. रोगाबद्दल समजावून सांगितले.
एक गोष्ट स्पष्ट झाली होती – जर महांतेशवर लवकर शस्त्रक्रिया केली गेली नसती नाही तर त्याचे खालच्या अंगांवर, मूत्राशयावर आणि आतड्यांवरील नियंत्रण जाणार होते हे नक्की होते. शस्त्रक्रिया धोक्याची होती पण केल्याशिवाय इलाज नव्हता.
मोठे वरदान
पण आमच्या कडे एक मोठे वरदान होते. मी काम करतो त्या समर्थ न्यूरो आणि सुपरस्पेशालिटी हॉस्पिटलमध्ये सर्जिकल नेव्हिगेशन सिस्टीम आहे जी मेंदू आणि मणक्याच्या शस्त्रक्रियांमध्ये खूप उपयुक्त असते.. महांतेशच्या गाठी लहान होत्या आणि त्यांना अचूक पणे काढण्याची गरज होती. सर्जिकल नेव्हिगेशन उपकरणे मला त्याच्या ट्यूमर शोधण्यात आणि त्याच्या सभोवतालच्या रीढ़ की हड्डीच्या ऊतींना इजा न करता फक्त ट्यूमर काढण्यास मदत करणार होती. मी कमीतकमी कशेरुकाची हाडे काढून टाकून अचूकपणे सर्जरी करू शकलो असतो.
मी महांतेश आणि कुटुंबीयांना समर्थ हॉस्पिटलमध्ये असलेल्या सर्जिकल नेव्हिगेशनच्या अत्याधुनिक साधनांबद्दल सांगितले. सर्जिकल नेव्हिगेशन मला ट्यूमर शोधण्यात आणि त्यांना अचूकपणे काढण्यात कशी मदत करेल याबद्दल समजावून सांगितले. या साधनांमुळे ऑपरेशन यशस्वी होण्याची शक्यता खूप जास्त होती हे पण सांगितले.
महांतेश आणि त्याची पत्नी यांना अनेक प्रश्न होते. मी त्यांना उत्तरे दिली आणि त्यांच्या सर्व शंका दूर केल्या. मग ते आशावादी झाले. ते शस्त्रक्रियेसाठी इच्छुक होते. पण खर्चाबाबत प्रश्न होताच.
माझ्यासाठी हे ऑपरेशन करणे एक खास बाब होती. जवळजवळ सर्व न्यूरोसर्जन्सनी ऑपरेशन करण्यास नकार दिला होता आणि जवळजवळ सर्वांनी सल्ला दिला होता की शस्त्रक्रियेचा धोका फायद्यांपेक्षा कितीतरी जास्त आहे. पण तरीही मी ऑपरेशन करायला तयार होतो त्याचे एकच कारण म्हणजे सर्जिकल नेव्हिगेशन.
मी काम करत असलेल्या समर्थ न्यूरो आणि सुपर स्पेशालिटी हॉस्पिटलमधील सर्जिकल नेव्हिगेशन मार्गदर्शन प्रणालीमुळेच मी शस्त्रक्रियेचा धोका पत्करण्यास तयार होतो. ती प्रणाली मला इतर भागांना नुकसान न पोहोचवता अचूक शस्त्रक्रिया करण्यास मदत करणार होती.
सर्जिकल नेव्हिगेशनमुळे मी चीरा लहानात लहान घेऊ शकत होतो, म्हणून ऑपरेशनची जखम अगदी लहान होणार होती. नेमके कुठे कापायचे आणि काय काढायचे हे मला सर्जिकल नेव्हिगेशनचा संगणक व स्क्रीन सांगणार होता. सर्व माहिती अचूक मिळाल्यास शस्त्रक्रियेला वेळही खूपच कमी लागणार होता. याचा सर्वाचा परिणाम शस्त्रक्रियेनंतर कमी वेदना होणार होत्या आणि जलद गतीने जखम बरी होणार होती. संसर्गाची शक्यताही काहीशी कमी होती.
नेव्हिगेशनशिवाय…
शस्त्रक्रिया खूप जोखमीची होती. जर मी नेव्हिगेशनशिवाय ऑपरेशन केले असते, तर मला त्याच्या मणक्याचे एक किंवा अधिक स्तर काढून टाकण्यास भाग पडले असते ज्यामुळे शस्त्रक्रियेदरम्यान आणि नंतर गुंतागुंत होण्याची शक्यता होती.
शस्त्रक्रियेचा दिवस
अंतेश शेलीकेरी यांची आर्थिक स्थिती कमकुवत होती म्हणून आम्ही जेवढे शक्य होते तेवढ्या कमी शुल्कात शस्त्रक्रिया करण्याचे ठरवून त्याला लवकरात लवकर शस्त्रक्रियेसाठी तयार केले.
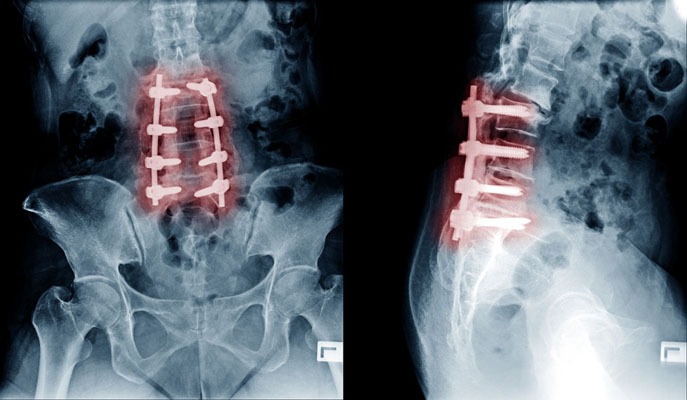
आमच्याकडे महांतेशच्या न्यूरोफिब्रोमाच्या सीटी स्कॅन आणि एमआरआय स्कॅन प्रतिमा होत्या. सी.टी. आणि एम.आर.आय. प्रतिमा संगणक प्रणालीमध्ये फीड केल्यानंतर आम्ही सर्जिकल नेव्हिगेशन प्रणाली सुरू केली. आम्ही नेव्हिगेशन सिस्टमचे ट्रॅकर्स महांतेशच्या पाठीवर अचूक ठिकाणी बसवले. आमच्या काही सर्जिकल उपकरणांमध्ये मार्कर असतात. अशा प्रकारे रुग्णांवर निश्चित केलेले मार्कर आणि आमच्या काही शस्त्रक्रिया उपकरणांवरील मार्कर सर्जिकल नेव्हिगेशन सिस्टमच्या 3D स्क्रीनवर स्पष्टपणे दिसू लागले. त्यामुळे आता नक्की कुठे कापायचे आणि कसे कापायचे हे कळत होते. या प्रतिमा आणि आमच्या कौशल्याच्या मदतीने आम्ही ऑपरेशन केले.
आम्ही ट्यूमरची पातळी अचूकपणे स्थानिकीकृत केली. मग ट्यूमर काढण्यासाठी आम्ही हाडांचा अचूक तुकडा काढला. आम्ही ड्युरामेटर [मेंदू आणि पाठीचा कणा यांचे कडक आवरण] उघडले आणि मी ती गाठ पाठीच्या कण्यापासून काळजीपूर्वक विच्छेदित केली. त्यानंतर मी T-12 आणि L-1 स्तरांमधील दोन्ही ट्यूमर तसेच L-2 पातळीच्या खाली असलेले ट्यूमर काढले.
आम्ही एकाच शस्त्रक्रियेत दोन्ही गाठी काढू शकलो. सर्वात महत्त्वाचे म्हणजे शस्त्रक्रिया यशस्वी झाली.
त्यानंतर शस्त्रक्रियेनंतरची काळजी आली. नर्सिंग केर आणि डॉक्टरांच्या राउंड व्यतिरिक्त फिजिओथेरपिस्ट हे एक अतिशय महत्त्वाचे काळजीवाहक होते. तिने महांतेशला हातपाय हलवायला प्रवृत्त केले आणि मार्गदर्शन केले कारण नसांवरील गाठींचा दाब कमी झाला होता. महांतेशला आश्चर्य वाटले की तो पाय हलवू शकतो. हे लक्षात घ्या की जेव्हा तो माझ्याकडे आला तेव्हा त्याने त्याचे खालचे हातपाय हलवण्याची क्षमता गमावली होती.
केवळ खालचे अंग हलवण्यापासून ते चालता येण्यापर्यंतची प्रगती महांतेशसाठी अवघड पण गरजेची होती. पण त्याने ते पूर्ण केली आणि वॉकरचा आधार घेऊन त्याला चालता आले. पण आपण खूप पुढच्या काळात जात आहोत…
त्या आधी समर्थ हॉस्पिटलमधून महांतेशला डिस्चार्ज मिळाला. शस्त्रक्रियेनंतर सातव्या दिवशी आम्ही त्याला डिस्चार्ज दिला. नेव्हिगेशनच्या सहाय्याने केलेल्या शस्त्रक्रियेमुळे त्याची जखम खूपच लहान होती. त्यामुळे त्याला जखमेच्या ड्रेसिंगची फारशी गरज नव्हती. त्याच्या शस्त्रक्रियेने झालेल्या जखमा लवकर बऱ्या झाल्या.
हे लिहितोय तेव्हा महांतेशला डिस्चार्ज होऊन बरेच महिने उलटले आहेत. शेलीकेरी दाम्पत्य बेळगाव येथे राहतात आणि त्यामुळे त्यांना भेटीसाठी येणे खूप दूर पडते. बेळगावमधील स्थानिक डॉक्टर महांतेशच्या रोजच्या समस्यांची काळजी घेतात.
पण महांतेशच्या पत्नी सौ. शेलीकेरी यांनी मला अनेक महिन्यांनी फोन करून महांतेशची प्रगती चांगली होत असल्याचे सांगितले.
आमच्या प्रयत्नांमुळे आम्ही महांतेशला पुन्हा चालण्यास मदत करू शकलो. मी देवाला आशा करतो की त्याला त्याच्या मणक्यावर किंवा इतर कोठेही न्यूरोफिब्रोमेटोसिसच्या गाठी पुन्हा येऊ नयेत.
शल्यक्रियेमुळे शेलीकेरी कुटुंब आत्ता सुखात आहे.